

Reflecting on HITECH and incentives for a better healthcare system
What we've learned about turning dollars into better patient outcomes


👋 Hello to our 1410 subscribers, including over 100 of you who joined last week!
This week we’re shifting gears back to healthcare policy and reflecting on the HITECH Act of 2009 — the landmark legislation that drove healthcare digitization in the 2010s.
In 2009, the global economy was struggling. Fresh off a historic election, President Obama spurred Congress to act on efforts to bring the economy back to life. A crown jewel of his legislative agenda was the Health Information Technology for Economic and Clinical Health Act, aka the HITECH Act.
HITECH wanted to encourage the widespread adoption and meaningful use of health information technology. The idea was that better health IT would make healthcare better in five concrete ways:
it would improve care quality and efficiency
improve patient engagement and care coordination
improve population health
reduce costs
ensure patient privacy and security
And HITECH had teeth: it provided $35 billion in incentives to upgrade health IT infrastructure and adopt electronic health records (EHR) while placing penalties for non-compliance.
With meaningful incentives in place, hopes were high that healthcare would improve significantly throughout the 2010s.
Smash cut to 2023, and it’s clear that HITECH was a mixed success:
“We put a big slug of money trying to encourage everybody [in healthcare] to digitalize and catch up with the rest of the world. And it's proven to be harder than we expected partly because everybody has different systems that don’t talk to each other.”
— former President Barack Obama in an interview with Vox in 2017, a few days before his second term ended.
Healthcare is still not working for millions of Americans. Government intervention may happen again. So what have we learned from HITECH that can help us do better next time?
Here are our five principles for better healthcare:
Focus on desired outcomes, not operations & procedures
Incentivize excellent physician and patient experiences
Foster a marketplace of better, faster, and more customizable solutions
Support an ecosystem of interoperable healthcare services
Standardize and implement healthcare APIs that can level the playing field between incumbents and newcomers
Outcomes, not process
HITECH’s major flaw was its fixation on process.
Its bet that better healthcare IT would result in better healthcare was correct — but how these goals translated into incentives was flawed.
The implicit assumption was that simply having digital records or EMRs would organically lead to better patient care. So the incentivizes were to implement an EMR, not the EMR that could make life better for healthcare workers or patients.
In the years to come, the deepest pockets drove how EMRs were purchased, designed, and implemented. HITECH unwittingly created incentives for consultants, healthcare facility firms, and finance teams to choose the lowest-priced or most easily accessible EMR solutions. Today, EMRs are primarily treated as billing tools — above all, they make sure insurance companies and hospital admins get paid, with care team and patient experience as an afterthought. To be clear, payments were way more frustrating before EMRs, but designing EMR UX should not be a zero-sum game between payors, providers, and patients.
The next HITECH should focus on implementation frameworks that reduce ambiguity, measure impact, and track progress on the outcomes we want to incentivize. Designing policy around desired outcomes can help direct resources to the most effective interventions. Instead of putting in guidelines for processes and assuming that desired outcomes will happen, set a clear target for what healthcare needs to look like, and align incentives with measuring and meeting the KPIs that improve the day-to-day experience of healthcare workers and patients.
Let’s dig into some of those desired outcomes…
Incentivize better care experiences
Doctors notoriously hate their EMRs. They are cumbersome, frustrating, and time-consuming. Today, most physicians review the EMR only after they begin an in-person or telehealth consultation. Navigating an EMR lowers the quality of patient interactions and worsens patient engagement.
A doctor that clicks through the EMR 50+ times during a single patient visit is using their EMR but at the expense of the patient’s care experience.
Many healthcare experts also posit that EMRs do not support medical needs. The president of KLAS Research, Taylor Davis, articulated in a Stanford Medicine Symposium:
“A physician said ‘I can't trust this EMR because it’s still asking me to input whether infants are chewing tobacco….’ The challenge is today there are clinically stupid things in EMRs that are hurting the trust that physicians have in these systems.”
Patients suffer too — I’ll never forget the time I had a checkup and my physician never even made eye contact with me. Their back was turned, focused solely on entering data in the EMR.
EMR implementation is not straightforward:
EMR users (care teams) are not the buyers.
Buyers are more concerned about budgets than improving care.
As a result, EMR providers tend to design their solutions to meet the needs of buyers, not care providers. Costs, scale, and licensing get more priority over usability or critical medical requirements.
And yet research suggests that physician support for EMR systems is the single most important factor in their successful adoption:
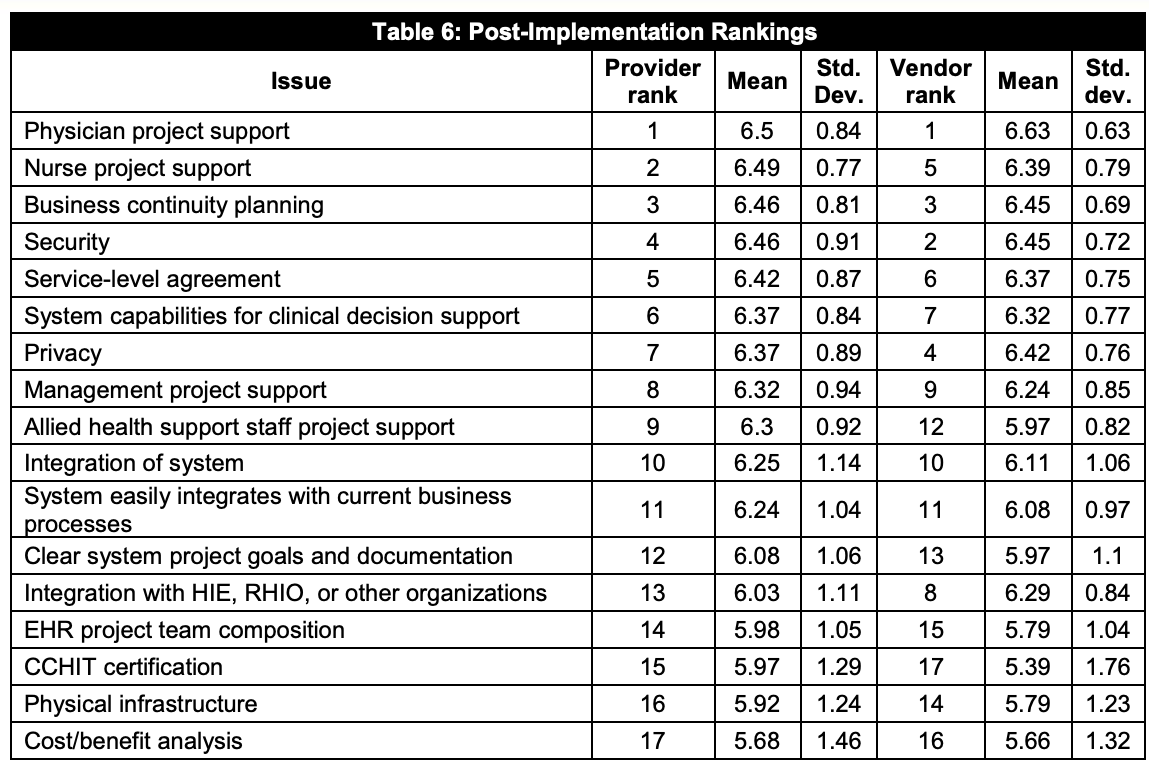
The next HITECH should balance decision-making power by making care teams’ (physicians, nurses, and PAs) and patients’ experience a core KPI.
EMR contract renewals and upgrades should be tied to important metrics such as user satisfaction, vendor responsiveness, and fixes for UX flows and bugs that impose an undue administrative burden.
While no software system is perfect, EMRs should natively integrate user feedback to lay the foundation for iterative improvement. By providing incentives for improving care experiences, we can help counter structural biases that prevent physicians from spending time with patients.
Enable a marketplace of better, faster, and customized solutions
No single software solution can meet the full diversity of patient needs and use cases. Specialties from pediatrics to geriatrics, family practice to highly specialized oncology treatments all demand their own flows.
Instead of one-size-fits-all EMR systems, the next HITECH can encourage more purposeful software, tailored to critical workflows, which are iteratively designed and improved based on user feedback.
Imagine a pediatric EMR solution that has a built-in pediatric diabetes protocol and automatically lists the most active seasonal flu for a region. Such a platform would greatly enhance the effectiveness of pediatric care.
Specialized software provides more customization and automation than broad, general tools. They can materially reduce the manual data-entry work that is burning out care teams, and catalyze more patient engagement opportunities.
Recent advances in language modeling will support the personalization of healthcare, as these services become smaller and more customizable.
Other industries like manufacturing, retail, and fintech have already fostered open marketplaces that encourage teams to iteratively develop products based on specific customer needs. It’s time that we encourage more customer-centric and feedback-responsive products.
Create an ecosystem of interoperable healthcare services
Promoting standards and incentivizing interoperable implementations for the storage and exchange of medical records beyond the EMR will create an improved ecosystem of healthcare services.
The HITECH Act led to EMRs designed for billing. As a result, we had data standards for CMS payments before we had standards for storing and exchanging patient medical records. It wasn’t until 2020 that health plans participating in federal exchanges needed to share claims data with patients electronically (thanks to the ONC Cures Act Final Rule).
To fully realize the value of digital health records, we need to be able to exchange data across all healthcare systems. A patient’s medical records, entered three years ago by a family physician, must be available today when they consult with a specialist.
Interoperability standards like FHIR are addressing data exchange. And the Office of the National Coordinator for Health Information Technology has followed on the heels of HITECH by encouraging adoption. Before their involvement, FHIR implementation was largely done voluntarily while facing headwinds from institutional players.
But gaps remain. Not all systems are fully able to make use of information in notes, scans, reports, and other unstructured data. Manually cleaning, labeling, and contextualizing medical records is a cumbersome and time-intensive process. The next HITECH can provide resources to make the most of all data in the EMR, especially care workflows that create or rely on text and images.
Standardized healthcare APIs will level the playing field
The next HITECH should also support interoperability and patient care by supporting technology implementation of standards.
In his assessment of HITECH’s shortcomings, President Obama also pointed out:
“[we have] economic incentives that are pushing against making the system work better. For example, there are service providers that make money on keeping people’s medical records — so making it easier for everybody to access each other’s medical records means that there’s some folks who could lose business, and that has turned out to be more complicated than I expected.”
The future of healthcare is APIs. Incentivizing the creation of healthcare APIs built on data storage and exchange standards can wrestle the data advantage away from the hands of large incumbent medical records service providers. Further, it can enable new players to tap into an ecosystem to create new solutions tailored to the long tail of challenging healthcare workflows.
Data is the currency of healthcare. More equitable, innovative, and patient-centric healthcare services will rely on solutions having secure, private, and consented access to data.
Though we spent most of this post focused on what to get better next time, it’s also important to acknowledge what went right — we learned that financial incentives work (sometimes too well), and healthcare is capable of digital transformation on a massive scale (despite a lot of derision from technologists outside healthcare).
Meaningful use and data entry incentives in HITECH led to a measurable decrease in adverse events, encouraged the creation of patient portals and secure messaging systems, led to better patient access to health records, and led to the rise of health information exchanges to improve care coordination and support decision-making.
Though simply having EMRs may not solve all problems, it lays the foundation for understanding how healthcare can be better, and how we can learn from each patient’s experience.
Now that we can learn from our healthcare data, we can point future financial efforts toward the right targets.
Thanks for reading,
Alda & Gaurav 🌊
Great piece, really highlights a lot of the issues with HCIT Information Systems, I found this comment particularly insightful:
"In the years to come, the deepest pockets drove how EMRs were purchased, designed, and implemented. HITECH unwittingly created incentives for consultants, healthcare facility firms, and finance teams to choose the lowest-priced or most easily accessible EMR solutions. Today, EMRs are primarily treated as billing tools — above all, they make sure insurance companies and hospital admins get paid, with care team and patient experience as an afterthought. To be clear, payments were way more frustrating before EMRs, but designing EMR UX should not be a zero-sum game between payors, providers, and patients."
The future of healthcare are APIs 👏